

DHEA Deficiency, in Family Practice
The incidence of DHEA deficiency in a family practice: symptoms observed and the effects of supplementing serum DHEAS

FIRST, THREE CAVEATS
(1) Please allow me, before going any further, to recognise and admit that this is an anecdotal, retrospective report, regarding an unfiltered, un-organized population which attended a family practice ad hoc, between 2006 and 2021, at the time, there was no plan to report the findings and no control of time of presentation. Particularly, this was not a double-blind study.
This report therefore, is presented as an opinion piece, which (hopefully), some scientifically-inclined researcher may find thought-provoking and worthy of in-depth, scientific investigation.
(2) Some of the graphics herein were taken from previous publishings and their enumeration may seem inappropriate: please consider correct., the enumeration in the text.
(3) I report on 585 individuals – 266 men and 359 women, but this post shares detail regarding the men only – the women’s symptomatology was very complicated and would have rendered this article much too long: their stories will be reported in a separate post, in July, 2025.
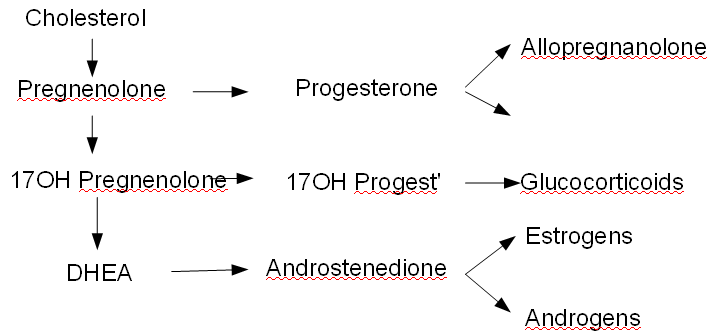
Fig 1: Genesis and metabolism of DHEA
585 documented patients: 226 males and 359 females
I have analysed the records of 585 patients, to the point of detailing my therapeutic success in the management of 226 males; but the 359 female patients’ records are so much more complicated that my report re. therapeutic success with women cannot be readied for some months: I will complete it by mid-July 2025 and will submit it as a stand-alone post.
No concrete conclusions can be drawn from this record, regarding any aspect of DHEA deficiency, excepting for the salient points ……..
A sufficiently large subset of the patient population (in my family practice, 92% of females and 70% of males) needs investigation for DHEA insufficiency, to warrant advising family physicians to be aware of the problem and to prepare to diagnose and treat the condition.
Health Canada’s attitude toward hormone restoration in general and DHEA/Pregnenolone supplementation in particular, needs to change! It is time to remove these two side-effect free, supportive, all-important antiaging hormones, which have been freely available over-the-counter in the United States since 1995, from Canada’s “dangerous drugs” list.
At a minimum, we should educate our family practitioners on the subject of DHEA and DHEA deficiency and we should permit them to recommended supplementation appropriately.
At best, Canada should permit over-the-counter sales of DHEA and Pregnenolone: the result would be ASTRONOMICAL SAVINGS, for our publicly-funded healthcare system.
Background review
DHEA is a fat-soluble molecule, which you might call a “steroid ring”. It is produced in small amounts by the brains of all animals and in large amounts (more than all of our other hormones, put together) by the adrenal glands of the primates, including humans. It is the essential raw-material for production of neurosteroid hormones and its deficiency implies deficiency of Its “downstream products” (Fig. 1).
The active form of DHEA (Fig 2) is fat-soluble, but for transport in the blood, a sulphur atom is attached to it, producing water-soluble “DHEAS”.
DHEAS is delivered via the blood, to all cells in the body: on entering the cells, the Sulphur atom is removed and the molecule reverts to fat-soluble DHEA.
Within the cells, DHEA is modified, to produce Testosterone and a series of “micro-hormones”, different for each cell type, which each produces for its own use. Thus DHEA is not truly a “hormone”, because apart from its special action (blocking an enzyme called G6PD) to promote the death of cancer cells, it doesn’t make any changes by itself: it is simply raw material for neurosteroid * hormone production.
DHEA levels are high at birth, because the mother produces it in quantity during pregnancy and it crosses the placenta to the baby.
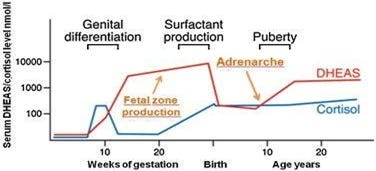
Levels fall rapidly after birth and remain low until puberty: at “Menarche” (girls) or “Adrenarche”(boys), between age 8 and 13 years, both genders maximise DHEA production (Fig. 3), keeping it high until age 25.
* “Neurosteroids” are hormones which are active in the brain and nerves.
Fig 3: Graphic from the excellent website, “you and your hormones”: Normal serum levels of DHEAS (red line), during pregnancy and up to age 20 – the curve for cortisol is included, because DHEA and Cortisol share the “root”, Pregnenolone (Fig1) The graphic shows DHEA in the male: in the female, DHEA levels are lower, but the trend is the same.
What DHEA does, for Humans
As the “prohormone” raw material for the neurosteroid hormones our cells (in particular, our brain cells) need, DHEA helps to keep function normal in all our organs. But starting at age 26, both men and women reduce production of this all-important prohormone, by 1% per year. So by the time we get to age 80, the production of DHEA is down to 10 % or less of what it was at 20 and eventually, the blood level hits Zero.
The basic cause of aging
This reduction of available DHEA is the root cause of many health complaints and is the basic cause of “aging”: the incidence of noncommunicable disease, including cancer, rises as DHEA fades away (see Figure 5).
The progressive loss of DHEA production and the gender difference are nicely documented by the “Normal DHEA” table with which test results were reported by “Life Labs”, in Canada, early in the 21st century – see Figure 4 and the associated “normal” table, below:
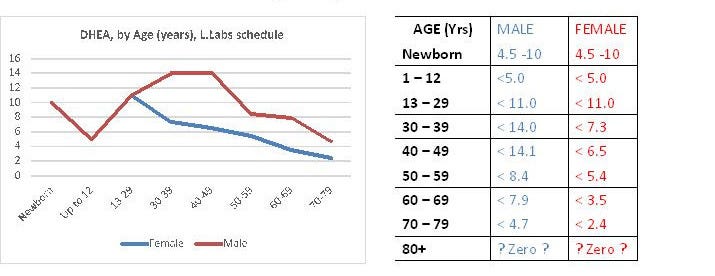
The 1%-per-annum diminution of DHEA production occurs in both sexes and begins at age 25. The rate of loss It is the same, regardless of the DHEA level at age 25 (the level at 25 is variable, because those who were stressed as children, or in the teen years, tend to produce less DHEA).
Note that women, who have lower serum levels in youth, tend to become deficient at an earlier age.
DHEA deficiency
When the serum level falls below 6.0 pmol per litre, symptoms of DHEA deficiency begin. Usually, women’s DHEA level falls to less than 6.0 micromoles per Litre at some point between 30 and 40 years of age, while men usually don’t cross that threshold until they are over 50……… However under stress conditions (especially in cases of childhood PTSD), aberrations of function due to subnormal DHEA supply can begin in the teen years.
The effect of childhood PTSD
When stress causes PTSD in childhood, Pregnenolone is “stolen”, to produce Cortisol instead of DHEA.
But that’s not all – not only is DHEA suppressed; cortisol decimates T3 production inside the cells, so the unfortunate child enters the teen years in a self-perpetuating state of combined DHEA deficiency and Intracellular Hypothyroidism.
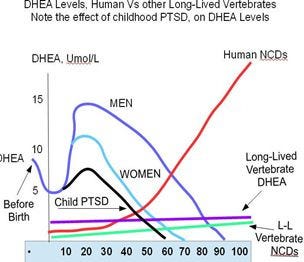
Figure 5: My clumsy modification of J.W. Nyce’s superb graphic shows the effect of PTSD on DHEA production. The blue (Male) and blue-green (Female) lines show humans’ DHEA level with age: Women’s levels fall below 6.0 by age 35-40, but Men’s DHEAS levels may exceed 6 pmol/L through age 60. The “lesser”, long-lived animals, producing DHEA only in the brain, have low, but steady, DHEA levels (purple line).
The red line shows our risk of cancer and other noncommunicable diseases, while the green one shows the liability to degenerative disease of long-lived mammals, who use other factors for protection from NCD’s.
The black line (my modification) shows the effect of childhood PTSD: serum DHEAS is reduced to less than 6 pmol/L by age 30 or earlier, and occasionally, in both girls and boys, may not even rise to 6.0 Pmol/L during the 2nd and 3rd decades.
DHEA deficiency
According to popular legend, as promulgated by our putative medical cognoscenti, the decline of DHEAS in our serum (Figures 4 and 5) is natural and therefore, the gradual disappearance of DHEA from our bodies constitutes neither deficiency, nor abnormality: by their tenets, it should be ignored.
